


 Sign Out
Sign Out


Pharmacology: Pharmacodynamics: Mechanisms of action and pharmacodynamic effects: Symbicort Turbuhaler contains budesonide and formoterol, which have different modes of action and show additive effects in terms of reduction of asthma and COPD exacerbations. The specific properties of budesonide and formoterol allow the combination to be used either as an anti-inflammatory reliever or as maintenance treatment for asthma, and for symptomatic treatment of patients with moderate to severe COPD (for 160/4.5 mcg only). The mechanisms of action of the two substances, respectively are discussed as follows.
Budesonide: Budesonide given by inhalation at recommended doses has a glucocorticoid anti-inflammatory action within the lungs, resulting in reduced symptoms and exacerbations of asthma with less adverse effects than when corticosteroids are administered systemically. The exact mechanism responsible for this anti-inflammatory effect is unknown.
Formoterol: Formoterol is a selective β2 adrenoceptor agonist that produces relaxation of bronchial smooth muscle in patients with reversible airways obstruction. The bronchodilating effect sets in rapidly, within 1-3 minutes after inhalation, and has a duration of 12 hours after a single dose.
80/4.5 mcg: Symbicort maintenance and reliever therapy: In studies of 6-12 months duration in patients from 4 years of age, as-needed use of Symbicort Turbuhaler, as an addition to a maintenance dose, was compared to treatment with the same maintenance dose of Symbicort or a 2-4 fold higher dose of budesonide, both with terbutaline as needed. Improved asthma control was seen from the first days of treatment, and the improvement was greater than that seen in the comparator treatments. Patients took, on average, 1 as-needed Symbicort inhalation per day and achieved statistically and clinically significant reductions in severe exacerbations and improvements in lung function and symptoms. These improvements were achieved with lower inhaled and oral steroid load than in the comparator treatments. There was no sign of attenuation of the anti-asthmatic effect over time.
A short-term study in patients experiencing an acute asthma attack has shown no difference in lung function improvements during the first three hours between treatment with Symbicort Turbuhaler and salbutamol pMDI + spacer.
Symbicort maintenance therapy: Clinical studies have shown that the addition of formoterol to budesonide improved asthma symptoms and lung function, and reduced exacerbations. The effect on lung function of Symbicort, given as a maintenance dose only, was equal to that of budesonide and formoterol in separate inhalers in adults and exceeded that of budesonide alone in adults and children. All treatment arms used a short acting β2 adrenoceptor agonist as needed. There was no sign of attenuation of the anti-asthmatic effect over time.
In a 12 week paediatric study, 85 children aged 6-11 years were treated with Symbicort (2 inhalations of 80/4.5 micrograms/inhalation twice daily), which improved lung function and was well tolerated.
160/4.5 mcg: Asthma: Symbicort anti-inflammatory reliever therapy: A total of 8064 patients aged 12 and above with mild asthma were included in 2 double-blind efficacy and safety studies (SYGMA 1 and SYGMA 2), of which 3384 patients were randomised to Symbicort anti-inflammatory reliever therapy for 12 months. Patients were required to be uncontrolled on only short-acting β2 agonist (SABA) as needed or controlled on low dose ICS or leukotriene receptor agonist plus SABA as needed.
Both studies compared Symbicort anti-inflammatory reliever therapy (Symbicort Turbuhaler 160/4.5 mcg used as needed in response to symptoms) to budesonide Turbuhaler 200 mcg (1 inhalation twice daily) given with as needed SABA. SYGMA 1 also compared Symbicort anti-inflammatory reliever therapy to as needed SABA alone.
In SYGMA 1 and SYGMA 2, respectively, based on physician assessment before enrolment, 44.5% and 46.3% of patients were uncontrolled on SABA as needed, and 55.5% and 53.7% of patients were controlled on low dose ICS or leukotriene receptor antagonists plus SABA as needed. At baseline, patients in SYGMA 1 and SYGMA 2, respectively, had a median age of 40 and 41 years (overall range across both studies 12 to 85 years), 12.5% and 9.8% of patients were adolescents (≥12 to <18 years) and approximately 7% and 9% of patients were over 65 years of age, 87.0% and 84.3% had never smoked, 10.3% and 13.1% were former smokers, 2.7% and 2.6% were current smokers, and 19.7% and 22.0% of patients had experienced a severe exacerbation within the 12 months prior to study enrolment.
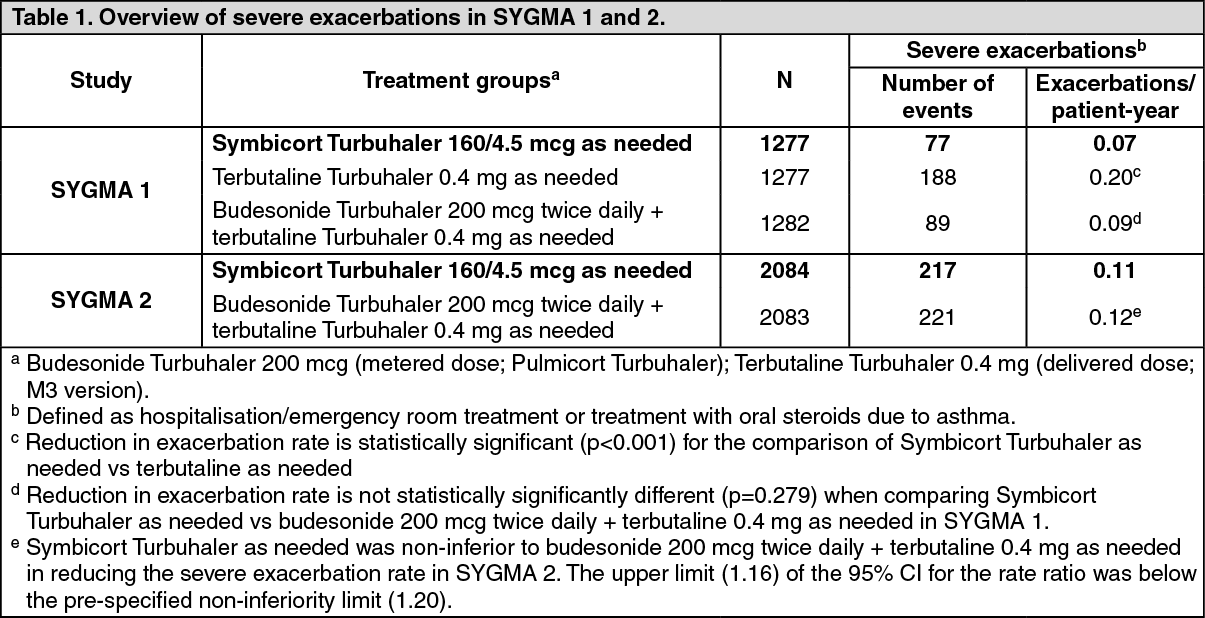
In SYGMA 2, Symbicort anti-inflammatory reliever therapy was comparable to a maintenance dose of budesonide Turbuhaler given with as-needed SABA in terms of the rate of severe exacerbations (Table 1). Protection against severe exacerbation was achieved with a 75% reduction in median ICS load and without requiring adherence to maintenance ICS treatment. SYGMA 1 showed that Symbicort anti-inflammatory reliever therapy provided a statistically significant and clinically meaningful reduction in the rate of annual severe exacerbations by 64% compared with SABA as needed alone (Table 1). Reduction in the annual rate of moderate to severe exacerbations was consistent (60%) with that observed for severe exacerbations (Risk Ratio (RR): 0.40 (95% Confidence Interval (CI): 0.32, 0.49); p<0.001).
In SYGMA 1, Symbicort anti-inflammatory reliever therapy provided superior daily asthma symptom control compared to as-needed SABA alone (Odds Ratio (OR): 1.14 (1.00 to 1.30); p=0.046), showing a mean percentage of weeks with well-controlled asthma of 34.4% and 31.1%, respectively. Asthma symptom control was inferior for Symbicort anti-inflammatory reliever therapy compared to a maintenance dose of budesonide Turbuhaler given with as-needed SABA (OR: 0.64 (2-sided 95% CI 0.57, 0.73; lower limit of the CI ≥0.8 for non-inferiority), showing a mean percentage of well-controlled asthma weeks of 34.4% and 44.4%, respectively. Improvements in asthma control (as defined by Asthma Control Questionnaire (ACQ-5)) in patients using Symbicort anti-inflammatory reliever therapy were superior to improvements in patients using as needed SABA alone (estimate for difference: -0.15 (-0.20, -0.11); p<0.001). In accordance with the pre-specified hierarchical testing strategy, apart from well-controlled asthma weeks, all other efficacy results from this study were considered of nominal statistical significance. Improvements in asthma control were lower for Symbicort anti-inflammatory reliever therapy compared to a maintenance dose of budesonide Turbuhaler given with SABA as needed (SYGMA 1 estimate for difference: 0.15 (0.10, 0.20); SYGMA 2: 0.11 (0.07, 0.15); both p < 0.001). For both comparisons, mean differences in treatments' effect upon ACQ-5 are not clinically meaningful (as assessed by a difference of greater than or equal to 0.5). These results were observed in a clinical study setting with considerably higher adherence to budesonide maintenance dosing than expected in real life.
In the SYGMA studies, increases in lung function compared to baseline (mean pre-bronchodilator FEV1) were statistically significantly larger for patients on Symbicort anti-inflammatory reliever therapy compared to patients on as needed SABA alone. Statistically significantly smaller increases were observed for Symbicort anti-inflammatory reliever therapy compared to a maintenance dose of budesonide Turbuhaler given with SABA as needed. For both comparisons, mean differences in treatments' effect were small (approximately 30 to 55 mL, equating to approximately 2% of the baseline mean).
Overall, the results of the SYGMA studies show that Symbicort anti-inflammatory reliever therapy is a more effective treatment than SABA as needed in patients with mild asthma. In addition, these studies suggest that Symbicort anti-inflammatory reliever therapy may be considered an alternative treatment option for patients with mild asthma who are eligible for ICS treatment. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAnalysis of time to first severe exacerbation in SYGMA 1 showed that the likelihood of experiencing a severe exacerbation was statistically significantly higher for SABA as needed use compared to Symbicort anti-inflammatory reliever therapy over the 1 year treatment period, with a risk reduction of 56% (Hazard Ratio (HR): 0.44 (0.33, 0.58); p<0.001). There were no differences in the probability of experiencing a severe exacerbation between Symbicort anti-inflammatory reliever therapy and a maintenance dose of budesonide given with SABA as needed.
Symbicort anti-inflammatory reliever plus maintenance therapy: The safety and efficacy of Symbicort in the Symbicort anti-inflammatory reliever plus maintenance therapy regimen have been investigated in six clinical trials using two dose strengths (80/4.5 and 160/4.5 mcg) of Symbicort Turbuhaler in patients with asthma. A total of 14219 patients (1134 elderly, 11144 adults, 1595 adolescents and 345 children) were randomised into the studies, of which 5514 were treated with Symbicort anti-inflammatory reliever plus maintenance therapy. Of the overall patient population 7% were smokers. In comparison with the usual patient proportions seen in practice, smokers and the elderly were under-represented in the trials. However, the results for these subgroups were generally consistent with the results for the whole study population. Patients with COPD were excluded.
The studies showed that Symbicort anti-inflammatory reliever plus maintenance therapy was significantly superior compared with fixed dose combination products or higher doses of ICS with a separate short acting or long acting β-agonist used as reliever (see Table 2 and Table 3). In the 5 double-blind long-term studies, patients receiving Symbicort anti-inflammatory reliever plus maintenance therapy used no reliever inhalations on 57% of treatment days and 0-2 reliever inhalations on 87% of treatment days. (See Tables 2 and 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image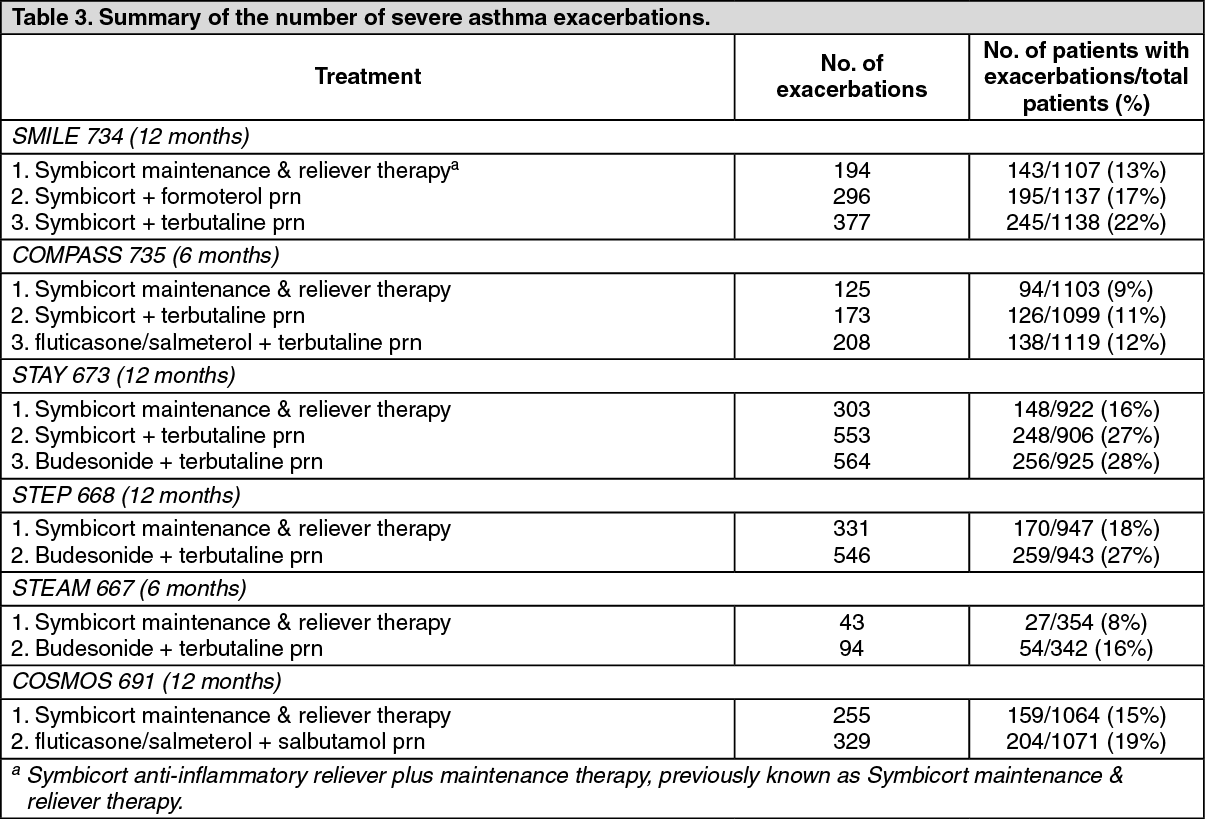 Click on icon to see table/diagram/image
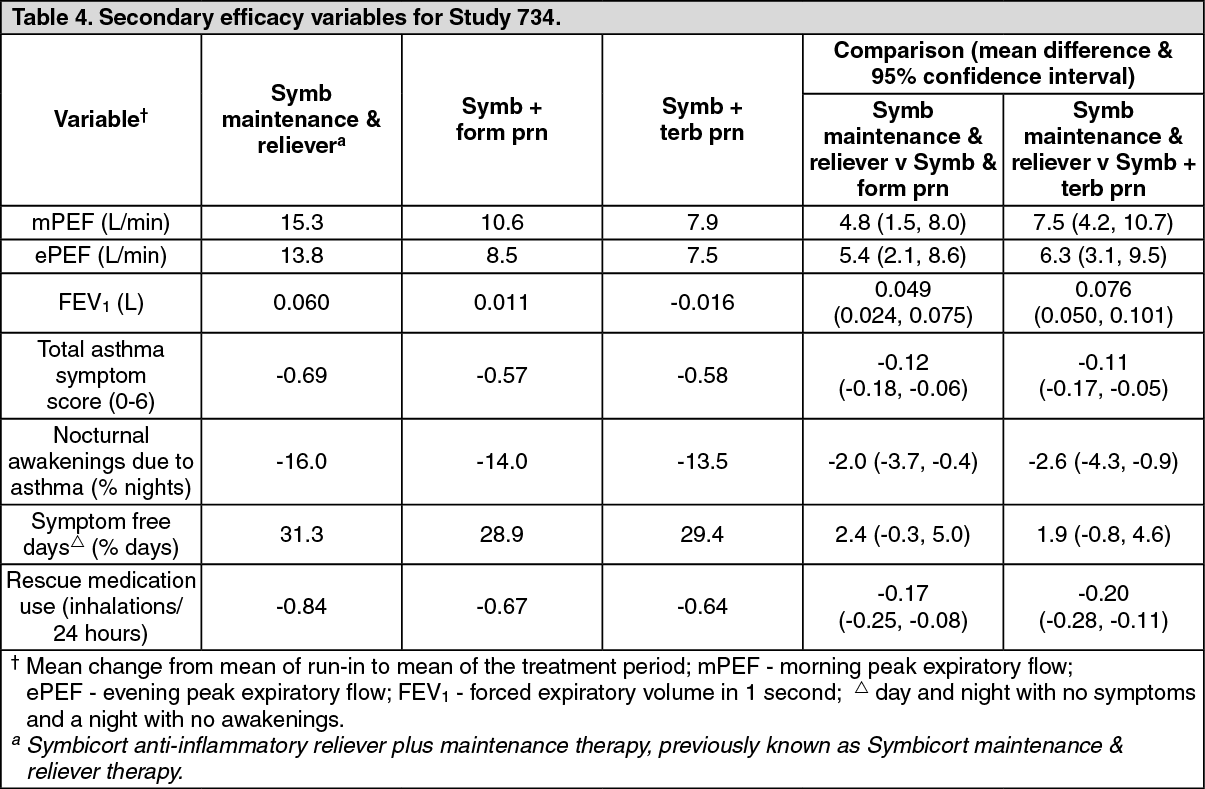
Click on icon to see table/diagram/imageStudy 734 (SMILE): A 12-month randomised, double-blind, parallel-group, trial in 3394 adult and adolescent patients aged 12 to 89 years with moderate to severe asthma. The study comprised of the following three arms: Symbicort anti-inflammatory reliever plus maintenance therapy: Symbicort Turbuhaler 160/4.5 mcg, 1 inhalation twice daily plus additional inhalations as needed.
Symbicort Turbuhaler 160/4.5 mcg, 1 inhalation twice daily with formoterol Turbuhaler as needed.
Symbicort Turbuhaler 160/4.5 mcg, 1 inhalation twice daily with terbutaline Turbuhaler as needed.
The primary efficacy variable, time to first severe exacerbation, was significantly increased with Symbicort anti-inflammatory reliever plus maintenance therapy compared with Symbicort plus formoterol and Symbicort plus terbutaline (see Table 2).
Use of oral steroids due to exacerbations was lower in the Symbicort anti-inflammatory reliever plus maintenance therapy group (1204 days total vs 2063 and 2755 days in the Symbicort plus formoterol and Symbicort plus terbutaline groups, respectively).
The majority of secondary variables supported the superiority of Symbicort anti-inflammatory reliever plus maintenance therapy over both comparators (see Table 4). The average daily as needed use in the Symbicort anti-inflammatory reliever plus maintenance therapy group was 1.02 inhalations/day and the frequency of high as-needed use was lower for Symbicort anti-inflammatory reliever plus maintenance therapy compared to both comparators. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe study specifically demonstrates that both the budesonide and the formoterol components of Symbicort Turbuhaler contribute to improved asthma control achieved through the as-needed dosing of Symbicort Turbuhaler within the Symbicort anti-inflammatory reliever plus maintenance therapy concept.
Study 735 (COMPASS): A 6-month randomised, double-blind, parallel-group trial in 3335 adult and adolescent patients aged 11 to 83 years. The study compared the following three arms: Symbicort anti-inflammatory reliever plus maintenance therapy: Symbicort Turbuhaler 160/4.5 mcg, 1 inhalation twice daily plus additional inhalation as needed.
Fluticasone/salmeterol Inhaler 125/25, 2 inhalations twice daily with terbutaline Turbuhaler as needed.
Symbicort Forte Turbuhaler 320/9 mcg, 1 inhalation twice daily with terbutaline Turbuhaler as needed.
The primary efficacy variable, time to first severe exacerbation, was significantly increased with Symbicort anti-inflammatory reliever plus maintenance therapy compared with both fluticasone/salmeterol plus terbutaline and Symbicort at a higher maintenance dose plus terbutaline (see Table 2).
Use of oral steroids due to exacerbations was lower in the Symbicort anti-inflammatory reliever plus maintenance therapy group compared to fluticasone/salmeterol plus terbutaline and Symbicort plus terbutaline (619 days total use vs. 1132 and 1044 days, respectively).
Results for secondary variables, including lung function, mean use of as-needed medication and symptom variables, were not significantly different between Symbicort anti-inflammatory reliever plus maintenance therapy and the other two groups. The average daily as-needed use in the Symbicort anti-inflammatory reliever plus maintenance therapy group was 1.02 inhalations/day.
Since the mean daily dose in the Symbicort anti-inflammatory reliever plus maintenance therapy group remained lower than in the Symbicort plus terbutaline group, the study specifically confirms the benefit of as-needed administration of part of the Symbicort dose.
Study 673 (STAY), Study 668 (STEP) and Study 667 (STEAM): In Studies 673, 668 and 667, Symbicort anti-inflammatory reliever plus maintenance therapy prolonged the time to the first exacerbation compared to Symbicort at the same maintenance dose with terbutaline as reliever and compared to a 2 to 4-fold higher maintenance dose of budesonide with terbutaline as reliever (see Table 2). Symptoms and reliever use were reduced and lung function improved compared with all other treatments (see Table 5, Table 6 and Table 7).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
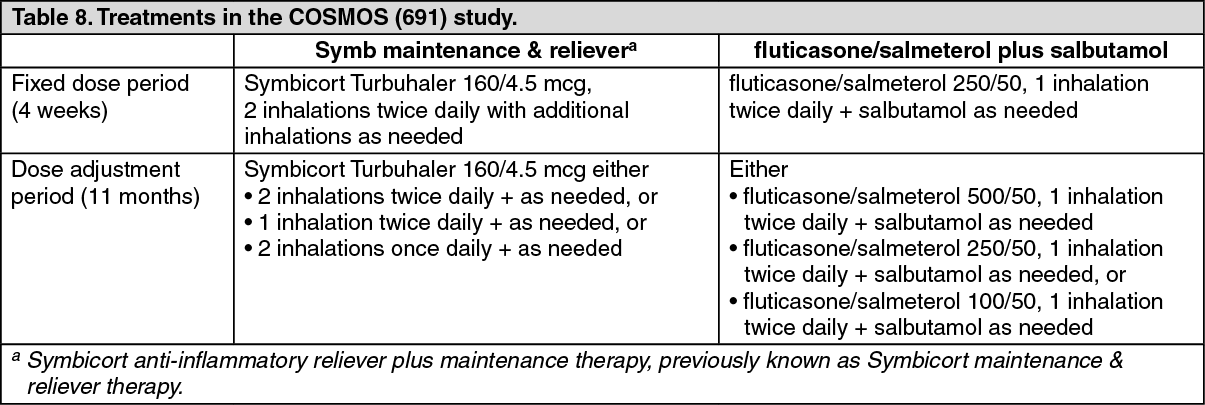
Click on icon to see table/diagram/imageStudy 691 (COSMOS): A 12-month, randomised, open, parallel group trial that compared the effectiveness of Symbicort anti-inflammatory reliever plus maintenance therapy with Seretide plus Ventolin in steroid-treated adult and adolescent patients (N=2143) aged 12 to 84 years with asthma. Randomised treatment started with a 4-week period during which the maintenance doses were fixed, followed by 11 months where the maintenance dose was adjusted to the lowest dose required for symptom control (see Table 8).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThis study showed that Symbicort anti-inflammatory reliever plus maintenance therapy treatment is more effective than adjustable therapy with fluticasone/salmeterol plus salbutamol in controlling asthma in adults and adolescents. Symbicort anti-inflammatory reliever plus maintenance therapy increased the time to first severe asthma exacerbations, reduced the total number of severe asthma exacerbations (see Table 2 and Table 3), reduced use of oral steroids for severe asthma exacerbations, and reduced use of as needed medications as compared with fluticasone/salmeterol at a similar daily ICS dose.
Safety in the combined studies: Symbicort anti-inflammatory reliever plus maintenance therapy treatment has a safety profile that is similar to budesonide and Symbicort maintenance therapy with a decrease in asthma-related adverse events.
Exercise-induced and allergen-induced bronchoconstriction: The use of Symbicort Turbuhaler 160/4.5 mcg in relation to exercise-induced and allergen-induced bronchoconstriction has been studied in three clinical trials for patients with mild/intermittent asthma.
Study D5890L00032 was a 6-week, 3-arm study in 66 adults and adolescents with mild asthma and episodic exercise-induced bronchoconstriction, in which the primary variable was change in maximum decrease in post-exercise FEV1 calculated before and after 6 weeks of treatment. This study demonstrated that Symbicort Turbuhaler 160/4.5 mcg, taken as 1 inhalation before exercise plus additional inhalations as needed in response to symptoms, improved asthma control by reducing exercise-induced bronchoconstriction to the same order of magnitude as regular maintenance treatment with budesonide 400 mcg plus terbutaline 0.5 mg as needed, despite a substantially lower steroid dose. Both treatments were superior to terbutaline as needed when taken alone.
Study AF-039-0001 was a 6-month, 2-arm study in 92 adults and adolescents with mild intermittent asthma who used SABA for symptom relief, in which the primary variable of efficacy was the change in level of fractional exhaled nitric oxide (FENO) in the two treatment groups over the duration of the study. This study demonstrated that the budesonide component in Symbicort Turbuhaler 160/4.5 mcg taken before exercise and as needed, reduced airway inflammation and improved airway function, and showed the beneficial effect of the budesonide component when taken as needed together with formoterol (for symptom relief) as Symbicort Turbuhaler 160/4.5 mcg.
Study D5890L00007 was a 3-arm, placebo-controlled, cross-over study in 15 adult patients with mild allergic asthma, in which the primary efficacy variable was change in PD20 (the provocative dose causing a 20% fall in FEV1) methacholine (MCh) during each treatment period. This study showed that when administered 30 minutes after a low-dose allergen challenge, Symbicort Turbuhaler 160/4.5 mcg abolished allergen-induced components of asthma deterioration whilst improving baseline pulmonary function, whereas, formoterol 6 ug alone inhibited the rise in symptoms but did not protect against allergen-induced airway inflammation. This study indicated that deteriorating asthma, provoked by low-dose allergen, is managed more effectively with Symbicort Turbuhaler 160/4.5 mcg than with formoterol.
Symbicort maintenance therapy: The efficacy and safety of Symbicort Turbuhaler for maintenance therapy has been evaluated in seven randomised, double-blind, double-dummy, active controlled, parallel group studies. All treatment arms in these studies used a SABA for relief of symptoms. Six studies were conducted for 12 weeks (80/4.5 and 160/4.5 presentations) while the 320/9 presentation study was conducted for 24 weeks (12 weeks efficacy and additional 12 weeks safety). Efficacy and safety data were collected for 3340 mild to moderate/severe asthmatic patients (2411 adults, 128 adolescents, 801 children aged 4 to 11 years old); 1704 were treated with Symbicort Turbuhaler.
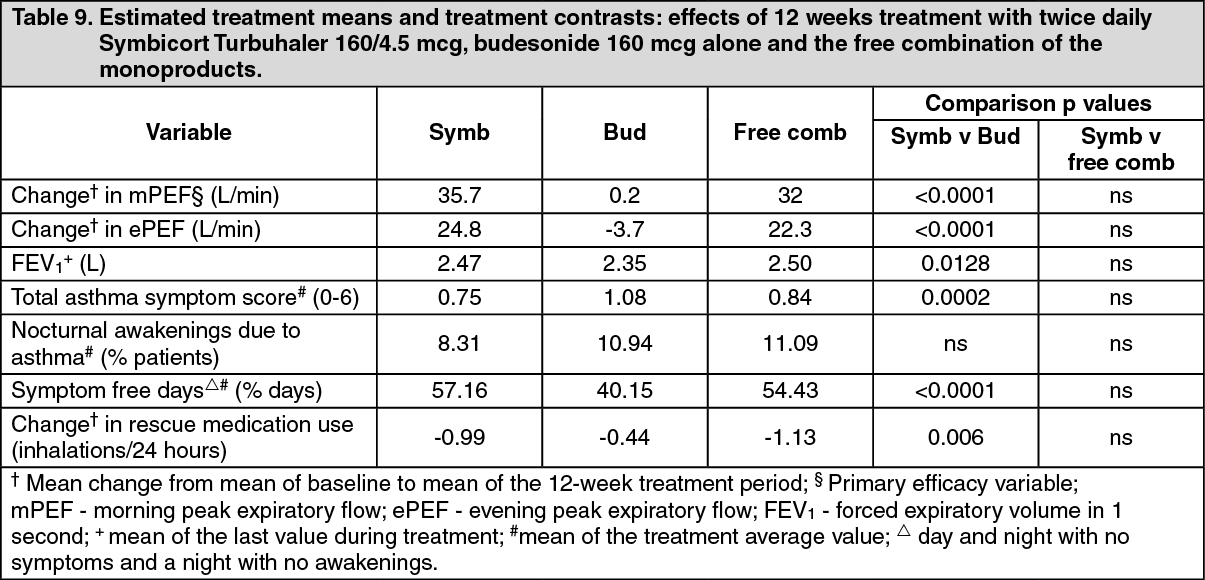
Symbicort Turbuhaler 160/4.5 mcg: In one study, the maximum recommended maintenance dose of Symbicort Turbuhaler 160/4.5 mcg (2 inhalations twice daily) was compared to corresponding doses of the free combination (budesonide Turbuhaler 200 mcg + formoterol Turbuhaler 6 mcg, two inhalations twice daily) and budesonide Turbuhaler 200 mcg (2 inhalations twice daily) only in adults with moderate asthma (mean FEV1 73.8% predicted normal and reversibility 22.5%). Table 9 details the efficacy results after 12 weeks treatment. (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageWhen administered twice daily, Symbicort Turbuhaler 160/4.5 mcg is a more effective treatment than budesonide, at corresponding budesonide doses.
320/9 mcg: Asthma: In clinical trials in adults, the additional of formoterol to budesonide improved asthma symptoms and lung function, and reduced exacerbations.
In two 12-week studies the effect on lung function of Symbicort Turbuhaler was equal to that of the free combination of budesonide and formoterol, and exceeded that of budesonide alone. There was no sign of attenuation of the anti-asthmatic effect over time. No clinical studies have been performed with Symbicort Forte Turbuhaler. Corresponding doses delivered with the lower strengths of Symbicort Turbuhaler are efficacious and well tolerated.
In a 12-week paediatric study 85 children aged 6-11 years were treated with Symbicort (2 inhalations of 80/4.5 micrograms/inhalation twice daily), which improved lung function and was well tolerated.
160/4.5 mcg and 320/9 mcg: COPD: In two 12-month studies, the effect on lung function and the rate of exacerbation (defined as courses of oral steroids and/or course of antibiotics and/or hospitalisations) in patients with moderate to severe COPD was evaluated. The inclusion criteria for both studies was pre-bronchodilator FEV1 <50% predicted normal. Median post-bronchodilator FEV1 at inclusion in the trials was 42% predicted normal.
The mean number of exacerbations per year (as defined previously) was significantly reduced with Symbicort as compared with treatment with formoterol alone or placebo (mean rate 1.4 compared with 1.8-1.9 in the placebo/formoterol group). The mean number of days on oral corticosteroids/patient during the 12 months was slightly reduced in the Symbicort group (7-8 days/patient/year compared with 11-12 and 9-12 days in the placebo and formoterol groups, respectively). For changes in lung-function parameters, such as FEV1, Symbicort was not superior to treatment with formoterol alone.
Pharmacokinetics: Absorption: Symbicort Turbuhaler and the corresponding monoproducts have been shown to be bioequivalent with regard to systemic exposure of budesonide and formoterol. In spite of this, a small increase in cortisol suppression was seen after administration of Symbicort compared to the monoproducts. The difference is considered not to have an impact on clinical safety.
There was no evidence of pharmacokinetic interactions between budesonide and formoterol.
Pharmacokinetic parameters for the respective substances were comparable after the administration of budesonide and formoterol as monoproducts or as Symbicort Turbuhaler. For budesonide, AUC was slightly higher, rate of absorption more rapid and maximal plasma concentration higher after administration of the fixed combination. For formoterol, maximal plasma concentration was similar after administration of the fixed combination. Inhaled budesonide is rapidly absorbed and the maximum plasma concentration is reached within 30 minutes after inhalation. In studies, mean lung deposition of budesonide after inhalation via Turbuhaler ranged from 32 to 44% of the delivered dose. The systemic bioavailability is approximately 49% of the delivered dose.
In children aged 6-16 years, lung deposition fall in the same range as in adults for the same given dose, the resulting plasma concentrations were not determined (for 80/4.5 mcg only).
Inhaled formoterol is rapidly absorbed and the maximum plasma concentration is reached within 10 minutes after inhalation. In studies the mean lung deposition of formoterol after inhalation via Turbuhaler ranged from 28-49% of the delivered dose. The systemic bioavailability is about 61% of the delivered dose.
Distribution and metabolism: Plasma protein binding is approximately 50% for formoterol and 90% for budesonide. Volume of distribution is about 4 L/kg for formoterol and 3 L/kg for budesonide. Formoterol is inactivated via conjugation reactions (active O-demethylated and deformylated metabolites are formed, but they are seen mainly as inactivated conjugates). Budesonide undergoes an extensive degree (approx. 90%) of biotransformation on first passage through the liver to metabolites of low glucocorticosteroid activity. The glucocorticosteroid activity of the major metabolites, 6-beta-hydroxy-budesonide and 16-alfa-hydroxy-prednisolone, is less than 1% of that of budesonide. There are no indications of any metabolic interactions or any displacement reactions between formoterol and budesonide.
Elimination: The major part of a dose of formoterol is transformed by liver metabolism followed by renal elimination. After inhalation, 8-13% of the delivered dose of formoterol is excreted unmetabolised in the urine. Formoterol has a high systemic clearance (approximately 1.4 L/min) and the terminal elimination half-life averages 17 hours.
Budesonide is eliminated via metabolism mainly catalysed by the enzyme CYP3A4. The metabolites of budesonide are eliminated in urine as such or in conjugated form. Only negligible amounts of unchanged budesonide have been detected in the urine.
Budesonide has a high systemic clearance (approximately 1.2 L/min) and the plasma elimination half-life after i.v. dosing averages 4 hours.
The pharmacokinetics of formoterol in children have not been studied (for 80/4.5 mcg only). The pharmacokinetics of budesonide or formoterol in patients with renal failure is unknown. The exposure of budesonide and formoterol may be increased in patients with liver disease.
Toxicology: Preclinical safety data: The toxicity observed in animal studies with budesonide and formoterol, given in combination or separately, were effects associated with exaggerated pharmacological activity.
In animal reproduction studies, corticosteroids such as budesonide have been shown to induce malformations (cleft palate, skeletal malformations). However, these animal experimental results do not seem to be relevant in humans at the recommended doses. Animal reproduction studies with formoterol have shown a somewhat reduced fertility in male rats at high systemic exposure and implantation losses as well as decreased early postnatal survival and birth weight at considerably higher systemic exposure than those reached during clinical use. However, these animal experimental results do not seem to be relevant in humans.